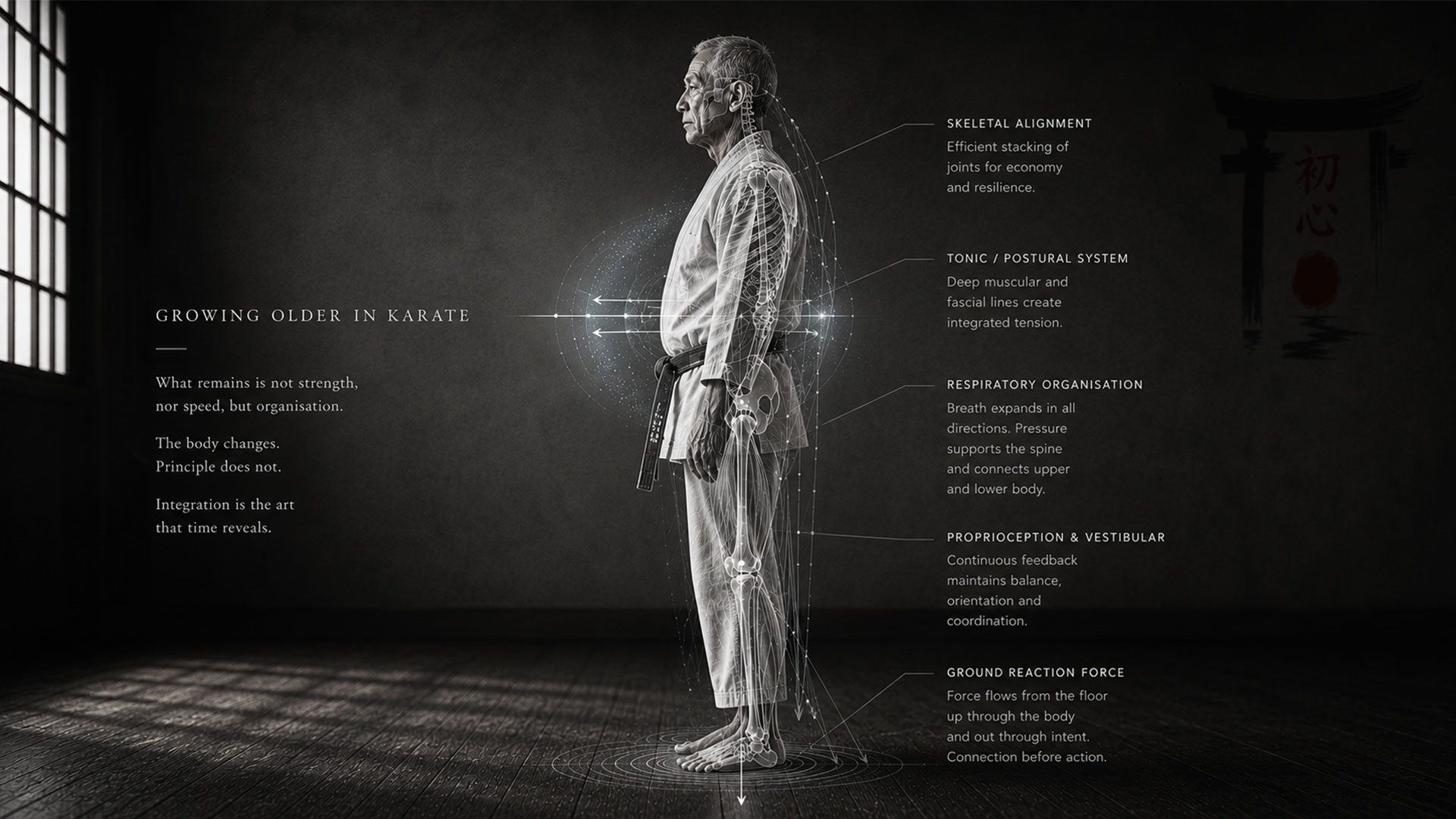
Growing older in Karate
…Ageing is not a choice, but you can choose how to age…
There comes a point in training when the body changes the rules. Not much at first. The techniques still work. The combinations are still familiar. Kata remains somewhere deep in the nervous system, appearing almost automatically once movement begins. But something shifts anyway.
You need longer to warm up. The hips and knees don’t forgive stupidity anymore. The shoulders tighten for no obvious reason. Ankles complain after movements that once felt effortless. Recovery stretches into the next day, then the one after that. And tension, especially the useless kind, starts accumulating faster than it used to.
Younger karateka rarely notice any of this. Speed and raw power compensate for any inefficiencies; fast recovery masks the signs of body abuse. Force generated locally works well enough. But as I began to feel it myself – the tightness, the slower recovery, joints complaining more than they used to – I started watching the older karateka more carefully. The ones who moved well looked different. Softer, less visibly athletic. Yet heavier in movement, more connected. Power arrived without visible strain.
Which raised the question: how were they managing what I was beginning to feel?
I used to think this was simply a matter of timing and experience compensating for declining capacity. That is certainly part of it. But it is also incomplete. Over the past years, I have been reading work on posture, fascia, breathing, nervous system regulation, and integrated movement that gave language to things many long-term practitioners already feel directly in training. Some of this work sits outside mainstream sports science. For karate, that matters.
Because the real question is not how to fight age, the real question is what is declining, why it matters for karate specifically, and what traditional training already does about it, often without the student fully understanding why.
What’s declining
The standard explanation for ageing in karate is simple: you lose strength, speed, and flexibility. The advice? Train harder, and you slow the decline. This is true as far as it goes, but it describes symptoms without explaining the mechanism (it’s a bit like saying a car slows down because the wheels turn less).
The deeper story begins with sarcopenia, the progressive loss of skeletal muscle mass that starts around age thirty and accelerates after sixty. Research consistently reports a decline of 3 to 8 per cent of muscle mass per decade after thirty, with the rate increasing significantly in later decades [1][2]. By eighty, the cumulative loss can reach 30 per cent or more [3]. Muscle strength and power decline even faster than mass itself [3].
But the loss is not uniform – and this is the part that matters for karate.
Your body maintains two functionally distinct muscle systems: tonic muscles and phasic muscles [4]. Tonic muscles are the deep stabilisers – slow-twitch fibres positioned close to the joints. They maintain posture, stabilise the spine, and work automatically below conscious awareness. Phasic muscles are the movers – fast-twitch fibres designed for powerful, rapid contractions that activate on demand then shut off [4][5].
Sarcopenia preferentially affects fast-twitch fibres [2][3], but the decline is not simultaneous across all systems. Tonic muscles, being slow-twitch and sensitive to disuse, weaken first and lose their reflexive activation early. Phasic muscles decline more slowly. In this window – often years or decades – the still-functional phasic system attempts to compensate for tonic loss. They take over stabilisation tasks they were never designed for. Because phasic muscles fatigue quickly and produce crude, large-scale contractions instead of the fine control that tonic muscles provide, the result is a body held together by tension and compensation. This manifests as elevated shoulders during kumite, a rigid lower back during stance transitions, and the inability to relax between techniques. The signs cascade through the whole body.
Four muscle groups are particularly important here, and their decline affects every aspect of karate practice. Understanding why these specific systems matter reveals the full scope of what ageing attacks.
The spinal stabilisers. When the multifidus (a set of deep, thin muscles running along the spine) weakens or loses its protective firing, the erector spinae (muscles running vertically on both sides of the spine, from the sacrum to the skull) compensate with total tightening [6][7]. The karateka develops a “strong” back that can deadlift heavy loads, but cannot maintain the segmental spinal control needed for a simple rotation in stance.
The gluteal complex. The gluteus maximus (the largest and most superficial muscle in the buttocks) is the primary engine of hip extension – the foundation of power generation in virtually every karate technique [8]. When it weakens, the pelvis destabilises, hip flexors tighten, and the lumbar spine compensates. The force that should originate from the floor and travel through the hips begins leaking at the pelvis, and the upper body works harder to make up the deficit.
The soleus. This deep calf muscle functions as the primary anti-gravity muscle of the lower leg [5]. For karate, the soleus (muscle situated in the calf) is the muscle that keeps you connected to the floor: it makes the constant micro-adjustments in stance that allow weight to shift smoothly through the feet [9][10].
The tibialis anterior (muscle situated on the lateral side of the shin). When this muscle weakens, foot clearance decreases, balance deteriorates, and falls become more likely. For older karateka, this translates directly into unstable stance transitions, compromised kicking mechanics, and the gradual loss of the barefoot sensitivity that traditional karate training depends on [8].
These four groups share something important: they all decline early, quietly, and with cascading consequences. The decline does not announce itself. It arrives as stiffness that takes longer to shift, as balance corrections that arrive a little bit late, as techniques that feel heavier than they should, as a growing sense that the body is working harder for diminishing returns.
The karateka who is told to “train harder” in response to these changes is being told to drive faster with the steering wheel failing.
The Integration Problem
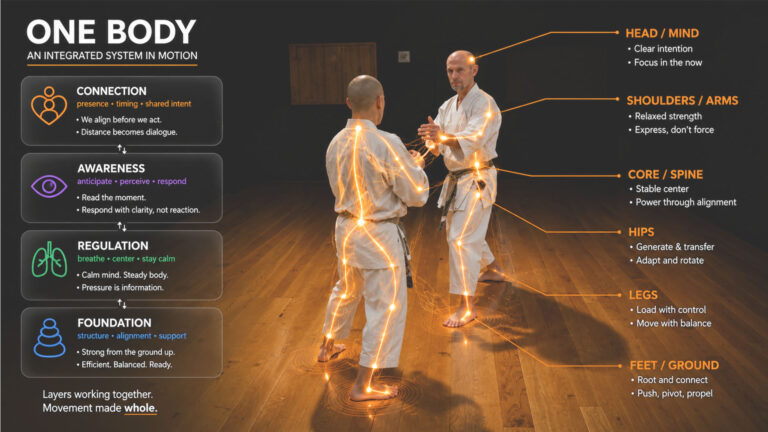
Many karateka reach a point in training when the body seems to work in disconnected sections. The shoulders try to generate power independently of the hips. The legs stabilise but do not actively contribute to movements above. Breathing feels separate from movement. The body fragments. Is this just a coordination issue? Not quite. It reflects something structural – the way the body is organised.
I explored this architecture in detail in “The Continuous Web“. The body is a tensional network: continuous chains of fascia link structures across multiple body regions, with bones floating within that web as compression elements. Force travels through these chains, not through individual muscles. A 2026 in vivo study by Colonna et al. confirmed this directly, demonstrating measurable force transmission along the posterior spiral chain from the latissimus dorsi (“lats”) through the thoracolumbar fascia (fascia that covers the lower back region) to the contralateral gluteal region [13]. Stretching one end of the chain altered the trunk rotation range of motion at the other.
For karate, this has direct practical consequences. In gyaku-zuki, force originates from the floor and travels through connected fascial chains: foot, leg, hip, thoracolumbar fascia, trunk, and striking arm. An efficient technique uses the whole chain. This is what experienced practitioners mean when they talk about “body connection” or “using the whole body.” Whether consciously understood or not, they describe efficient force transmission through intact myofascial chains. This is why older karateka who move well appear to generate power without visible effort. They are not producing force locally. They are transmitting it globally. The problem with ageing is that these chains degrade.
Fascia is a living, mechanically active tissue. It contains contractile cells (myofibroblasts) that can actively modify tissue tension, and it contains more sensory receptors than muscle tissue, making it one of the richest proprioceptive organs in the body [15]. Its mechanical properties depend heavily on hydration: dehydrated fascia stiffens, loses its capacity to slide and transmit force smoothly, and becomes less responsive to the subtle load variations that movement requires [12][15].
With age, fascia tends to become less hydrated, more fibrotic, and less elastic. The cross-links between collagen fibres increase. The sliding surfaces between fascial layers become less mobile. The result, experienced on the dojo floor, is the progressive loss of what practitioners call “flow/smoothness”: the feeling that movement passes through the body without obstruction. Techniques that once felt connected begin to feel segmented. A force that once arrived effortlessly now requires muscular effort to push through resistance that the karateka may not even be able to locate.
Add to this the proprioceptive dimension (the body’s internal sense of its own position, movement, and force). The multifidus, as described in the previous section, contains an exceptionally high density of muscle spindles. But the deeper rotatores muscles (the smallest of the transversospinales group) contain even higher spindle density [6][7]. These tiny muscles produce almost no movement. They exist primarily as sensory organs, reporting spinal position to the central nervous system with great precision. When they weaken or become inhibited through disuse, injury, or age, the karateka loses spinal position sense. The brain’s internal map of the spine becomes less accurate, and segmental control deteriorates. For karate, this loss of proprioceptive feedback eliminates the body’s capacity for fine segmental control during rotation and complex movement sequences.
This is what an ageing karateka often experiences when techniques feel “off” despite no obvious mechanical failure. The proprioceptive system that once guided spinal organisation during complex movement has degraded, and the conscious mind has neither the speed nor the resolution to compensate.
You can see this in kata. A younger student performing Bassai Dai moves through transitions with a certain unconscious precision: each vertebral segment contributing its share of rotation, the spine behaving as a connected chain. An older karateka whose deep stabilisers and proprioceptors have declined tends to rotate the trunk as a single rigid block. The movement looks similar from the outside. From the inside, and to an experienced eye, the quality is different. One is integrated. The other is stiffened.
Integration is not only about muscles and fascia; it deeply involves the nervous system and breathing mechanics, which together regulate movement quality and postural control.
The good news (and there is good news) comes in the sections ahead. Because traditional karate training, when properly understood and applied, is remarkably well designed to maintain specifically these systems. But before we get to what training does right, we need to address one more layer of the problem: breathing and the nervous system.
Breathing and the Nervous System
I discussed the nervous system’s role in movement regulation in “The Inner Web” and explored the integration of these layers in “One Body“. The central point, for our purposes here, is simple: the nervous system doesn’t just command movement – it reads the body’s tension, posture, and breathing patterns continuously, and adjusts its own state in response. A body held in chronic tension teaches the brain to remain on alert. A breathing pattern that never settles signals a threat. This loop – between body and brain – becomes harder to break with age. Here, I build on that foundation to address ageing in karate directly.
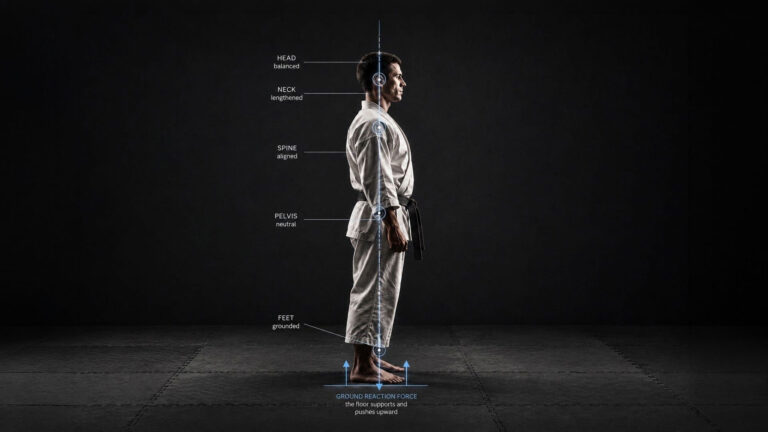
The diaphragm serves a dual function: it is both a primary breathing muscle and a key postural stabiliser. This dual role creates one of the most important dynamics in the entire movement system. When the diaphragm contracts during inhalation, it descends into the abdominal cavity, creating negative pressure in the chest (drawing air in) and positive pressure in the abdomen (pushing the organs down and outward). This increase in intra-abdominal pressure is one of the primary mechanisms of lumbar spine stabilisation [16].
Think of the trunk as a pressurised cylinder. The diaphragm forms the top, the pelvic floor the bottom, and the transversus abdominis wraps around the sides. When these three contract in coordination, they create a hydraulic column that supports the lumbar spine from within. This is true core stability: pressure-based, reflexive, and automatic – distinct from the voluntary abdominal bracing commonly promoted in fitness advice [16][17].
Kolar et al. demonstrated this effect using dynamic MRI synchronised with spirometry: during postural tasks, the diaphragm descends further into the abdominal cavity than during quiet breathing, increasing its stabilising contribution as the demands on the system rise [16]. The nervous system manages this automatically, allocating the diaphragm’s effort between breathing and stabilisation according to need. Problems arise when breathing becomes dysfunctional. The body will always prioritise breathing over stabilisation. If the karateka is a chronic chest breather, a mouth breather, or a habitual hyperventilator, the diaphragm cannot perform both roles simultaneously. Breathing wins. Postural support is sacrificed.
When this happens, the accessory breathing muscles (scalenes, sternocleidomastoid, upper trapezius, pectoralis minor) take over respiratory duties. These are muscles of the neck, chest, and upper back. Constantly used for breathing, they become tight and overactive: the head drifts forward, the shoulders round, the ribcage elevates into a fixed position. Physiotherapists often spend a long time trying to correct this postural pattern with stretches and strengthening exercises, without long-term success, because they are treating a downstream compensation while the upstream cause, dysfunctional breathing, remains unaddressed [17].
Any good karate instructor recognises this pattern. The student whose shoulders climb during combinations. The karateka whose neck visibly contracts during kata. The training partner who cannot maintain zanshin because the entire upper body is engaged in breathing by the third round of kumite. These are all expressions of the same underlying mechanism: the diaphragm has lost its postural role, and phasic muscles are compensating. This connects directly to the stress-posture feedback loop.
Stress, whether psychological or metabolic, produces a recognisable postural signature: rounded shoulders, collapsed chest, forward head, clenched jaw, shallow breathing. This is the flexion response, the same protective pattern that animals adopt when threatened [18]. The ventral surface (front part of the human body) closes down to shield the vital organs. The extensors along the back lose tone. The body makes itself smaller.
Research confirms that this relationship runs in both directions. Upright posture during stressful tasks has been associated with lower cortisol levels and greater emotional resilience. Slumped posture has been associated with increased sympathetic nervous activity and decreased parasympathetic tone [18][19]. The posture and the stress state reinforce each other in a continuous loop.
For the ageing karateka, this loop becomes increasingly difficult to break through effort alone. Chronic life stress (work pressure, family demands, accumulated injuries, poor sleep) keeps the body inclined toward flexion. The diaphragm cannot descend properly because the psoas (a long, deep core muscle connecting the spine to the legs) is pulling the lumbar spine forward. Breathing stays shallow. The nervous system reads the body’s own tension signals and maintains a low-grade alert state. Technical quality deteriorates in ways the karateka cannot pinpoint, because the source is not mechanical. It is regulatory.
This is why the emphasis that good karate teachers place on breathing is physiological, not mystical. Restoring full diaphragmatic movement resets the pressure dynamics of the trunk, releases the accessory breathing muscles from their compensatory role, improves oxygen delivery to working muscles through the Bohr effect (first described by Christian Bohr in 1904, where adequate CO₂ levels facilitate the release of oxygen from haemoglobin into tissues) [17][20], and shifts the nervous system toward parasympathetic dominance. A karateka who breathes well stands differently, moves differently, and recovers better. One who breathes poorly fights a system working against itself.
One observation from metabolic research is worth noting. Some researchers propose that cellular energy production – particularly mitochondrial efficiency and thyroid-mediated ATP regulation in skeletal muscle – directly affects the capacity of tonic postural muscles to maintain sustained low-level contraction [21]. If this is correct, chronic undereating, poor sleep, and prolonged metabolic stress do not simply cause fatigue. They degrade the energy supply to the very muscles responsible for upright posture and spinal organisation. Posture is as much a metabolic problem as a mechanical one. A practitioner who sleeps well, eats adequately, and manages stress has a structural advantage over one grinding through corrections on five hours of sleep and willpower.
With this understanding of the body’s complex systems, we can now see how traditional karate training methods align remarkably well with the needs of an ageing practitioner.
What Traditional Karate Already Does Right
This is where the picture comes together. When you examine traditional karate training through the lens of what the body needs to resist age-related decline, the match is remarkably precise. The “boring” work that younger students endure and older practitioners gravitate toward turns out to be targeted maintenance of exactly the systems described in the previous sections.
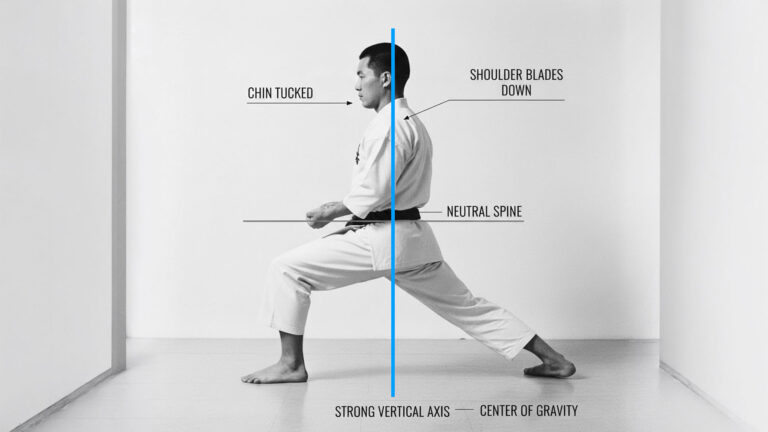
Stance work trains the tonic system. Holding zenkutsu-dachi, kokutsu-dachi, or kiba-dachi for extended periods is a sustained, low-intensity loading of the deep stabilisers. The multifidus must maintain segmental spinal control throughout. The transversus abdominis (horizontal “corset” that wraps around the torso from the ribs to the pelvis) and pelvic floor co-contract to stabilise the trunk. The soleus works continuously to manage balance through the feet. The gluteal complex stabilises the pelvis under load. This is tonic muscle training: slow-twitch fibre recruitment through sustained contraction, precisely the stimulus that maintains the postural system. Research confirms that low-intensity resistance exercise with slow movement and tonic force generation produces muscle size and strength gains comparable to high-intensity training, even in older adults aged 59 to 76 [22][23]. Traditional karate stance work has been doing this for centuries.
Kata trains fascial chains. A correctly performed kata is a continuous sequence of weight shifts, rotations, directional changes, and coordinated breathing through which force travels along the full length of the body’s myofascial connections. The slow, deliberate transitions that senior karateka favour are particularly valuable: they load the fascial system through a full range of motion under sustained tension, which is exactly the stimulus fascia needs to maintain hydration, elasticity, and sliding capacity [11][12]. Fast, explosive kata has its place, but for the ageing practitioner, the slow version is the more important training tool.
Barefoot training maintains foot and ankle proprioception. Karate is practised barefoot. This is intentional, not incidental. The soles of the feet contain dense concentrations of mechanoreceptors that feed spatial orientation data to the brain, the cerebellum, and the vestibular system (the system responsible for providing the brain with information about motion, head position, and spatial orientation) [24]. Modern shoes suppress this input. Barefoot stance work, controlled weight shifting, and feeling pressure move through the feet during kata provide continuous proprioceptive stimulus to the tibialis anterior, the soleus, and the intrinsic foot muscles. A 2022 study found that barefoot walking produced more stable balance recovery in older adults than shod walking during perturbation-based training [25]. The karateka who has trained barefoot for decades has been building this neural foundation without knowing it.
Slow kihon train deep stabilisers. The emphasis within traditional karate on slow, controlled kihon, where each technique is performed with full body connection at reduced speed, recruits the tonic system preferentially. Speed favours phasic muscles. Slow, sustained movement with continuous tension favours tonic muscles. When Sensei Rokah asks students to perform 10-20 gyaku-zuki in slow motion with full connection from floor to fist, he is prescribing deep stabiliser training in a form that no gym programme replicates, because the movement demands integrated chain activation, spinal segmental control, breathing coordination, and proprioceptive feedback simultaneously.
Breathing practice is diaphragm training. The coordinated exhalation on technique, the emphasis on abdominal breathing during kata, and the kiai: all of these train the diaphragm in its dual role. The karateka who learns to maintain intra-abdominal pressure while breathing through a sequence of techniques is training exactly the diaphragmatic stabilisation that Kolar’s research identifies as central to spinal support [16]. The common instruction to breathe from the hara is, in physiological terms, an instruction to prioritise diaphragmatic descent over accessory muscle recruitment. The practice predates the research by several hundred years.
Relaxation training counteracts the flexion response. The repeated emphasis on releasing unnecessary tension between techniques, on softening the shoulders, on finding calm between bursts of effort: this is nervous system regulation. The practitioner who can move from maximal effort to genuine relaxation within a single breath is training the transition from sympathetic to parasympathetic dominance [18][19]. This becomes increasingly valuable with age, as the stress-posture feedback loop described in the previous section becomes harder to break through effort alone. The older karateka who cannot relax is not simply wasting energy. The nervous system is locked in a state that actively degrades posture, breathing, and movement quality.
None of this is accidental. The traditional training methods evolved through centuries of empirical observation: teachers watching students, noticing what worked, refining the practice, passing it on. They did not have the vocabulary of tonic and phasic muscles, myofascial chains, or diaphragmatic intra-abdominal pressure. They had something arguably more valuable: direct observation of what produced effective, sustainable movement in the human body across a lifetime of practice.
The irony is that the aspects of traditional training most often dismissed by modern sports science as “outdated” or “inefficient” (static stances, slow basics, emphasis on breathing and relaxation, barefoot practice, repetitive kata at low intensity) are the elements that target the systems ageing attacks first. The older karateka who abandons these in favour of high-intensity interval training and explosive plyometrics is training the wrong system entirely.
What You Might Add
Traditional karate training covers a remarkable amount of ground. For most karateka, it genuinely is enough. What follows is not a list of gaps that must be filled, but a set of additions for those who want to supplement specific areas – particularly practitioners over forty who train less frequently than they’d like, or who notice particular weaknesses creeping in despite regular practice. None of this replaces dojo work. Think of it as targeted maintenance you can do in the margins of a busy week.
Hip extension work. Karate stances place an extensive load on the legs, but much of that load falls on the quadriceps and hip flexors. The gluteus maximus, despite its importance for power generation and pelvic stability, is often underworked in typical dojo training – not because training is deficient, but because the sustained hip extension that directly challenges the glutes occurs less frequently than the isometric holding of flexed positions. Walking lunges and deep split-stance movements, performed slowly and with full control, are among the most effective ways to load the glutes through a complete range of motion [8]. These can be integrated into a warm-up or performed on non-training days if you find your glutes aren’t firing as they should.
Spinal extensor maintenance. Kata and kihon train the spinal stabilisers isometrically during technique, but they rarely load the spinal extensors through their full range in isolation. For practitioners whose back feels persistently tight or who struggle with segmental control during rotation, simple prone extensions – lying face down, lifting the chest off the floor, holding for ten to thirty seconds – directly target the erector spinae and, when performed slowly and with segmental awareness, also target the deeper multifidus [6][7]. A Roman chair is useful (but not essential). Five minutes of controlled back extensions a couple of times a week can make a noticeable difference for those who need it.
Soleus and tibialis work outside the dojo. Barefoot training already maintains these muscles remarkably well. Many karateka will never need to add anything. But for those who notice declining balance or foot sensitivity, seated calf raises – bent-knee, targeting the soleus specifically – and tibialis raises – standing with back to a wall, lifting the toes toward the shins – are simple, low-equipment exercises that can be performed daily [9][10]. They can be done at a desk, on a phone call, or while waiting for the kettle. This is not a training programme – it’s a small addition for those who feel they’d benefit.
Fascial hydration and mobility. The sliding capacity of fascial layers depends on hydration and varied movement [15]. Karate training tends toward repetitive movement in familiar planes. For most people, it provides sufficient variety. If you train frequently and feel stiffness accumulating in patterns that kata doesn’t reach, an additional movement that takes the body through unfamiliar ranges – slow rotations, lateral bends, spiralling movements, gentle hanging, varied walking surfaces – can help. This does not need to be a structured gym class. Relaxed movement on non-training days is sufficient, if it feels necessary at all.
Recovery as training. Sleep, walking, gentle movement between sessions, and stress management are not supplements to training. For the older karateka, they are part of it. The nervous system does not distinguish between training stress and life stress. Both accumulate. Both affect posture, breathing, movement quality, and the capacity to access the deep stabilising systems that make technique work [18][19]. A student who trains hard three times a week and sleeps poorly every night is undermining the very adaptations the training is trying to produce.
Closing
The body ages. Joints stiffen. Recovery slows. Injuries leave their marks. Every karateka beyond a certain point feels this. Some warm-ups become negotiations with old damage. But what is actually declining is more specific – and more addressable – than the vague notion of “getting old.” The tonic stabilisers weaken. Fascial chains lose elasticity and hydration. Proprioception becomes less precise. The diaphragm loses its postural role. The nervous system drifts into patterns that hinder efficient movement. These are not vague complaints. They are identifiable systems with known mechanisms, responsive to the right stimulus at any age.
Traditional karate training, practised consciously with understanding, provides the stimulus. The stances, slow kihon, breathing, barefoot work, emphasis on relaxation, and patient, mindful repetition of kata are not just “tradition”. They are the targeted maintenance of the systems that the ageing attacks first. The older karateka who understands this is not training despite age. The training and ageing engage the same body, and the practice is designed for exactly this dialogue.
Karate practised over decades offers something unusual – the discovery that less force, better connection, and deeper understanding produce movement that is, in its own way, more complete than the athletic peak that preceded it. The body will age. The question is whether it ages into frailty or into something that still works.
Practical Summary
In the dojo: Prioritise slow stance work, controlled kata, barefoot basics, coordinated breathing, and conscious relaxation between techniques. Together, these simultaneously train the tonic stabilisers, fascial chains, proprioceptive system, and diaphragm.
Outside the dojo: Incorporate walking lunges to activate the glutes; prone extensions or Roman chair exercises for spinal extensors; seated calf raises for the soleus; and wall-supported tibialis anterior raises. Perform all exercises slowly, with sustained tension, two to four times per week.
Daily habits: Ensure adequate sleep, balanced nutrition, effective stress management, varied gentle movement on non-training days, and proper hydration. These are not optional extras – they form the metabolic foundation that supports the entire postural and stabilising system.
Author’s Note
This article represents my personal understanding and interpretation of traditional karate as taught by Hidetaka Nishiyama Sensei and followed by Avi Rokah Sensei. While I have endeavoured to accurately represent their teachings and methodology, any errors, misinterpretations, or misunderstandings are entirely my own. The insights and principles discussed here reflect my current level of comprehension as a student of this art, not the definitive word of my teachers.
Andrzej
This article may be shared, reprinted, or quoted for non-commercial purposes provided the author is credited and a link to the original article at nyuanshin.com is included. Commercial use requires prior written permission.
References
[1] Volpi E, Nazemi R, Fujita S. Muscle tissue changes with aging. Current Opinion in Clinical Nutrition and Metabolic Care. 2004;7(4):405-410. https://pmc.ncbi.nlm.nih.gov/articles/PMC2804956/
[2] Larsson L, Degens H, Li M, et al. Sarcopenia: aging-related loss of muscle mass and function. Physiological Reviews. 2019;99(1):427-511. https://pubmed.ncbi.nlm.nih.gov/30427277/
[3] Fielding RA, Vellas B, Evans WJ, et al. Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. Journal of the American Medical Directors Association. 2011;12(4):249-256. https://pmc.ncbi.nlm.nih.gov/articles/PMC3377163/
[4] Janda V. Muscles and motor control in low back pain: assessment and management. In: Twomey LT, ed. Physical Therapy of the Low Back. New York: Churchill Livingstone; 1987:253-278. Classification further discussed in: Page P, Frank CC, Lardner R. Assessment and Treatment of Muscle Imbalance: The Janda Approach. Human Kinetics; 2010.
[5] Comerford MJ, Mottram SL. Classification of muscles. In: Kinetic Control: The Management of Uncontrolled Movement. Churchill Livingstone/Elsevier; 2012. See also: Kolar P. Neural control and muscle fibre type classification. https://aneskey.com/classification-of-muscles/
[6] Multifidus dysfunction and chronic low back pain: systematic review and meta-analysis. International Journal of Spine Surgery. 2025;19(S3):S67. https://www.ijssurgery.com/content/19/S3/S67
[7] James G, Stecco A, Blomster L, et al. Muscle spindles of the multifidus muscle undergo structural change after intervertebral disc degeneration. European Spine Journal. 2022;31(7):1879-1888. https://link.springer.com/article/10.1007/s00586-022-07235-6
[8] VarianaVolk. 4 Muscles to Train for Maximum Anti-Aging Effect. The Race Lab Notes (Substack). March 2026. Underlying research on sarcopenia and glucose disposal reviewed in [1], [2], and [3].
[9] Hamilton MT, Hamilton DG, Zderic TW. A potent physiological method to magnify and sustain soleus oxidative metabolism improves glucose and lipid regulation. iScience. 2022;25(9):104869. https://pubmed.ncbi.nlm.nih.gov/36034224/
[10] Elek D, Tóth M, Sonkodi B, et al. The efficacy of soleus push-up in individuals with prediabetes: a pilot study. Sports. 2025;13(3):81. https://pmc.ncbi.nlm.nih.gov/articles/PMC11946342/
[11] Wilke J, Krause F, Vogt L, Banzer W. What is evidence-based about myofascial chains: a systematic review. Archives of Physical Medicine and Rehabilitation. 2016;97(3):454-461. https://pubmed.ncbi.nlm.nih.gov/26281953/
[12] Krause F, Wilke J, Vogt L, Banzer W. Intermuscular force transmission along myofascial chains: a systematic review. Journal of Anatomy. 2016;228(6):910-918. https://pmc.ncbi.nlm.nih.gov/articles/PMC5341578/
[13] Colonna S, Maietti G, Cuoghi F. In vivo evidence of myofascial force transmission along the posterior spiral chain: functional connectivity linking the contralateral latissimus dorsi, thoracolumbar fascia, and gluteal region. Cureus. 2026;18(1):e100760. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12867544/
[14] Levin SM. The icosahedron as a biologic support system. Alliance for Engineering in Medicine and Biology; 1981. See also: Swanson RL. Biotensegrity: a unifying theory of biological architecture. Journal of the American Osteopathic Association. 2013;113(1):34-52.
[15] Bordoni B, Marelli F, Morabito B, Sacconi B. A review of the theoretical fascial models: biotensegrity, fascintegrity, and myofascial chains. Cureus. 2019;11(1):e3875. https://pmc.ncbi.nlm.nih.gov/articles/PMC7096016/
[16] Kolar P, Sulc J, Kyncl M, et al. Stabilizing function of the diaphragm: dynamic MRI and synchronized spirometric assessment. Journal of Applied Physiology. 2010;109(4):1064-1071. https://journals.physiology.org/doi/full/10.1152/japplphysiol.01216.2009
[17] Kocjan J, Gzik-Zroska B, Nowakowska K, et al. Postural-respiratory function of the diaphragm assessed by M-mode ultrasonography. PLoS One. 2022;17(10):e0275389. https://pmc.ncbi.nlm.nih.gov/articles/PMC9550028/
[18] Nair S, Sagar M, Sollers J, Consedine N, Broadbent E. Do slumped and upright postures affect stress responses? A randomized trial. Health Psychology. 2015;34(6):632-641. https://doi.org/10.1037/hea0000146
[19] Wilkes C, Kydd R, Sagar M, Broadbent E. Upright posture improves affect and fatigue in people with depressive symptoms. Journal of Behavior Therapy and Experimental Psychiatry. 2017;54:143-149. https://doi.org/10.1016/j.jbtep.2016.07.015
[20] Bohr C, Hasselbalch K, Krogh A. Ueber einen in biologischer Beziehung wichtigen Einfluss, den die Kohlensäurespannung des Blutes auf dessen Sauerstoffbindung übt. Skandinavisches Archiv für Physiologie. 1904;16(2):402-412.
[21] Metabolic regulation of postural muscle function: see discussion in VarianaVolk. Your Posture Problem Is a Metabolism Problem. The Race Lab Notes (Substack). April 2026. Underlying thyroid-muscle physiology reviewed in: Salvatore D, Simonides WS, Dentice M, Zavacki AM, Larsen PR. Thyroid hormones and skeletal muscle. Endocrine Reviews. 2014;35(2):233-264.
[22] Tanimoto M, Ishii N. Effects of low-intensity resistance exercise with slow movement and tonic force generation on muscular function in young men. Journal of Applied Physiology. 2006;100(4):1150-1157. https://journals.physiology.org/doi/full/10.1152/japplphysiol.00741.2005
[23] Watanabe Y, Madarame H, Ogasawara R, Nakazato K, Ishii N. Increased muscle size and strength from slow-movement, low-intensity resistance exercise and tonic force generation. Journal of Aging and Physical Activity. 2013;21(1):71-84. https://pubmed.ncbi.nlm.nih.gov/22832536/
[24] Korchi K, Noé F, Bru N, Paillard T. Enhancing foot somatosensory inputs by barefoot practice optimizes the effects of physical activity on plantar sensation and postural control in institutionalized older adults. Journal of Aging and Physical Activity. 2019;27:452-465.
[25] Peng HT, Song CY, Chen ZR, et al. Barefoot walking is more stable in the gait of balance recovery in older adults. BMC Geriatrics. 2022;22:924. https://pmc.ncbi.nlm.nih.gov/articles/PMC9700923/



Andrjez,
This really stayed with me. The way you talk about aging in karate felt like someone quietly naming things I’ve been feeling but never quite put into words. There’s a gentleness and honesty in what you wrote that made me pause — in a good way. It reminded me that the practice deepens even as the body changes, and that there’s a kind of grace in that. Thank you for capturing it so beautifully.
Bw
Steve
Steve, again, many thanks! We do age, but the choice – how – belongs to us. I wanted only to highlight what the process entails and what we can do about it.
Regards,
Andrzej
valyakorovina83@gmail.com